Hallux Abducto Valgus (or ‘bunion’ is an enlargement of the joint (a lump of bone) at the base of the hallux. Bunions are a valgus deviation of the hallux commonly associated with an exostosis on the 1st metatarsophalangeal joint (MTPJ).
Biomechanical Aetiology
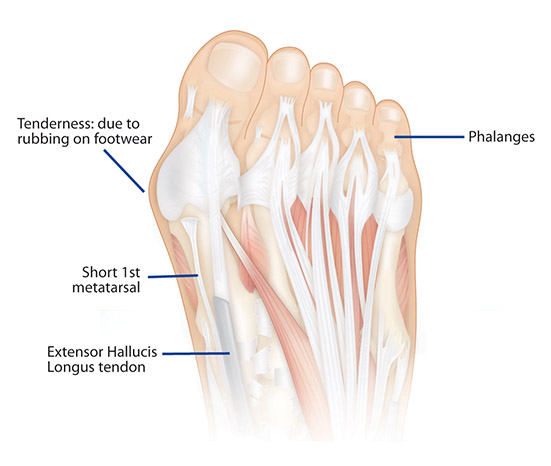
The main biomechanical factors in the development of a bunion are excess pronation of the subtalar joint, combined with a short 1st metatarsal.
As the foot pronates, the centre of gravity moves towards the midline, loading the forces on the medial forefoot area. This action puts excessive weight on the hallux during the toe off phase of gait, increasing the load on the 1st metatarsal shaft in an adductory direction, causing rotation of the shaft, which then causes the hallux to compensate by abducting. The hallux then deviates towards the lesser digits and the joint enlarges to accommodate the addition load.
Hallux Abducto Valgus (HAV) is not necessarily an entirely hereditary condition. Bunions can run in a family but it is the biomechanical structure (i.e. short 1st metatarsal and excessive pronation) that is hereditary and passed through the family – not the resultant condition itself. In some cases bunions are caused by arthritis or trauma. Fractures or breaks in the joint may lead to arthritic changes and the development of bunion deformities whilst limiting the range of motion in the joint.
Contrary to popular belief footwear is not the common cause of bunions. Although poor footwear in combination with causative biomechanical factors can cause bunions to develop quicker and progress further.
Hallux Abducto Valgus may be experienced in 3 stages: primary, secondary and tertiary. These stages refer to the progressive deviation of the hallux towards the midline of the body. Often, bunions in the tertiary stage cause the hallux to overlap or underlap the 2nd toe, usually limiting the patient’s mobility and causing pain.
Stages of Bunion Development: Primary > Secondary > Tertiary
HAV X-Ray
Symptoms
Pain may be felt in the 1st MTPJ, and a protruding lump on the medial side of the hallux, which enlarges with age. The skin and tissue around the bunion may also be swollen or inflamed, very painful or in some cases patients exhibit no pain at all. If left untreated the hallux will increasingly deviate until it reaches the tertiary stage, in which the big toe either overlaps or underlaps the 2nd toe. As a result, pain, discomfort and difficulty wearing shoes may be experienced due to the bunion deformity. Arthritis and stiffness in the joint can also develop.
The lesser toes can also be affected – pressure from the hallux pushing inward toward the lesser toes can cause toe nails to begin to grow into the sides of the nail bed or the smaller toes can develop corns. A ‘hammer toe’ may also develop in the 2nd toe due the deviation of the hallux.
Treatment
Primary and secondary stage bunions can be successfully treated with correctly fitted orthotics to realign and control the feet. ICB Orthotics moulded to the patient’s subtalar joint neutral position will assist in limiting excessive pronation, which in turn
re-distributes the body weight away from the 1st metatarso phalangeal joint during toe off reducing abduction of the hallux – ultimately preventing further development of the bunion.
ICB Orthotics control excess pronation reducing the load on the medial forefoot area and reducing valgus deviation of the hallux. ICB Orthotics re-establish proper weight distribution and lower limb
biomechanics which may prevent or reduce gradual growth of a bunion. If HAV is identified and treated with corrective orthotic devices, in the primary or secondary stages, this can assist in preventing further development of the bunion. Adding a Mortons Extension in the primary and secondary stages can assist in supporting the short 1st metatarsal and assist in the toe off phase of gait. To create a Mortons Extension an ICB Forefoot addition can be attached to the distal edge, with the medial edge being trimmed slightly to ensure an easy fit into the patient’s footwear.
Orthotic With a Morton's Extension
Additional Treatment
Sometimes surgery may be indicated when the bunion is at a tertiary stage, however ICB Orthotics should be worn after surgery to prevent any reoccurrence.