Lower Back and hip pain (non trauma related) can be attributed to many underlying causative factors including: unilateral and bilateral pronation and functional and structural leg length discrepancies. It is important to accurately identify if there is a functional or structural leg length difference in patients suffering low back and/or hip pain, as the treatment regimes are different.
Biomechanical Aetiology
Low back pain is associated with excessive pronation occurs due to the pelvic cage rotating anteriorly causing a lordosis at L1 to L5 (‘sway back’) with excessive stress in that area.
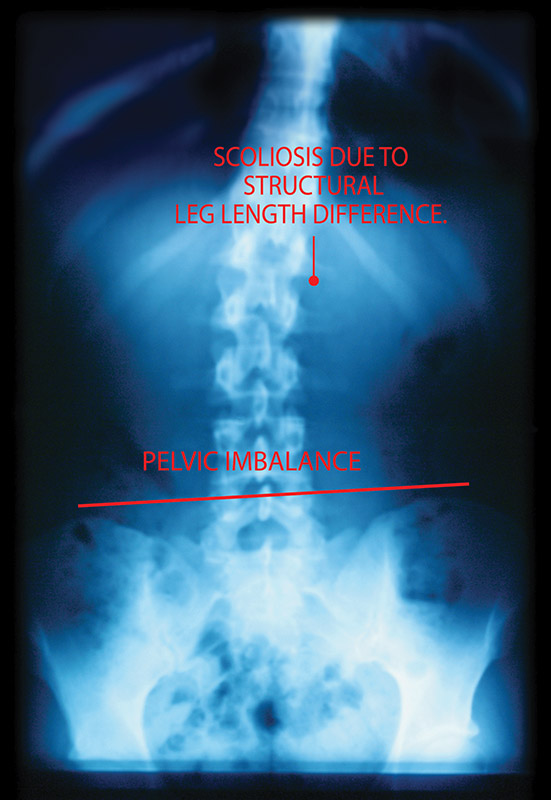
A structural leg length discrepancy is as the name suggests, a difference in the measurement of the tibia and femur, and can be hereditary or trauma-related. A structural leg length difference can result in the longer leg jamming up into the hip and Sacro-Illiac joint.
A functional leg length discrepancy can arise from a variety of causes including soft tissue compensations and trauma, which can affect the biomechanics of the body. Soft tissue compensation can occur to muscular imbalance (arising from, for example, poor training techniques) or maybe due to habit (for example, lying on one side in bed).
Both structural and functional leg length differences are important to identify, especially when low back or hip pain are present. Both types, if left untreated, can cause a predisposition to hip joint wear and tear on the longer leg side, and the need for a hip replacement later in life.